Product development guided by medical experts

An Open Clinical Trial of Glycoceramide-containing Cream and Lotion on Dry Skin of Atopic Dermatitis
Department of Dermatology, Kobe University School of Medicine 7-5-1 Kusunoki-cho, Chuo-ku, Kobe 650-0017, Japan
Tatsuya Horikawa, Tsutomu Takashima, Susumu Harada, Toshiya Chihara and Masamitsu Ichihashi
Key words: atopic dermatitis, ceramide, dry skin, water-keeping application, water content of corneum
We investigated the efficacy and usefulness of glycoceramide-containing cream and lotion, AK cream and AK lotion, on dry skin of atopic dermatitis. Marked improvement, moderate improvement or slight improvement was observed in 20 of 30 patients. Six patients were unchanged and 4 exacerbated. Usefulness of the agents was assessed according to the efficacy and safety index and proved to be 67%. We conclude that the glycoceramide-containing cream and lotion used in the present study are useful for the skin care of mild atopic dermatitis. Skin Research, 40: 415-419, 1998
■Introduction
The etiology of atopic dermatitis is not fully understood, but it is an allergic reaction1) whose onset is frequently and strongly associated with both hereditary and environmental factors. Exacerbation of atopic dermatitis is closely related to scratching, and the itching sensation is considered to be aggravated by the drying of skin. It has been shown that in atopic dermatitis, the water-retaining capacity of the stratum corneum is decreased2), and that the decrease is caused specifically by a reduction in the amount of sphingolipids, ceramides, which constitute intercellular space lipids of horny layer with cholesterol and fatty acids and a reduction of the natural moisturizing factor, composing mainly of amino acids3-6).
Most patients with atopic dermatitis have dry skin, which in turn augments the itching and is considered to be closely implicated in the exacerbation of the illness due to scratching. Meanwhile, it is generally accepted that the skin of atopic dermatitis patients is hypersensitive to external irritants. Ceramides have not only a water-retention function but also a barrier function on the skin to protect the internal structures of the body against external irritants, and their decrease reduces the effectiveness of the barrier function of the skin. Therefore, the topical application of ceramides should be useful in control of barrier funciton of atopic dermatitis. In the present clinical study , we found the efficasy of topical use of creams and lotions containing glycoceramide on the skin (especially on dry skin) of atopic dermatitis patients.
■Purpose and Methods
Purpose: We investigated the efficacy of creams and lotions containing glycoceramide on skin problems of atopic dermatitis patients (especially on the dry skin) in this study.
Methods: The subjects consisted of 30 patients with atopic dermatitis (8 mild, 16 moderate, 6 severe) who had been treated in the Department of Dermatology, Kobe University School of Medicine between June 1, 1996, and April 31, 1997. They received topical applications of 0.5% glycoceramide-containing cream (AK cream, Rosette Co., Ltd) or 0.85% glyceramide-containing lotion (AK lotion, Rosette Co., Ltd) two to three times daily. During the clinical study, other treatments were unchanged. Only three patients had received topical applications of steroids, without symptomatic changes, for over a month before the beginning of the study. We obtained the verbal consent of all the patients.
■Assessment
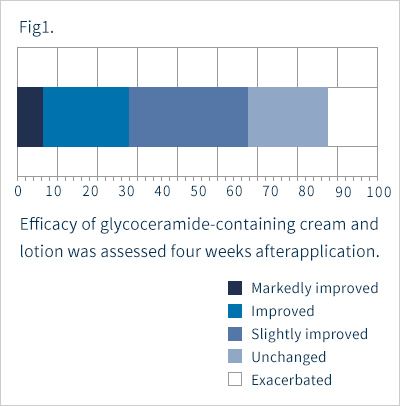
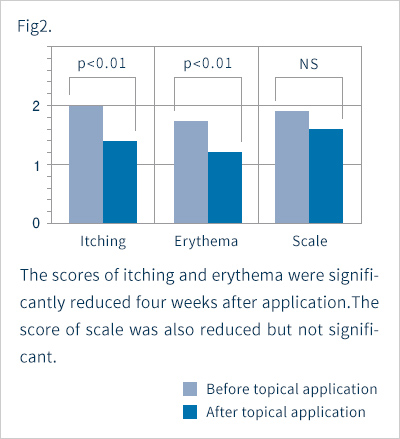
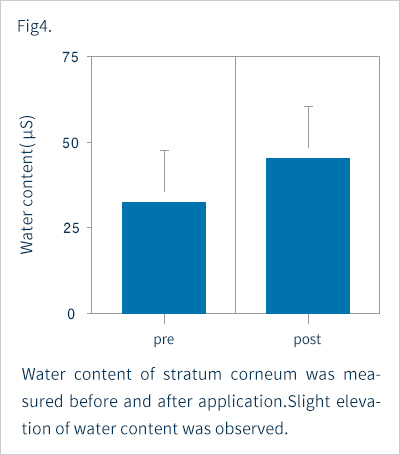
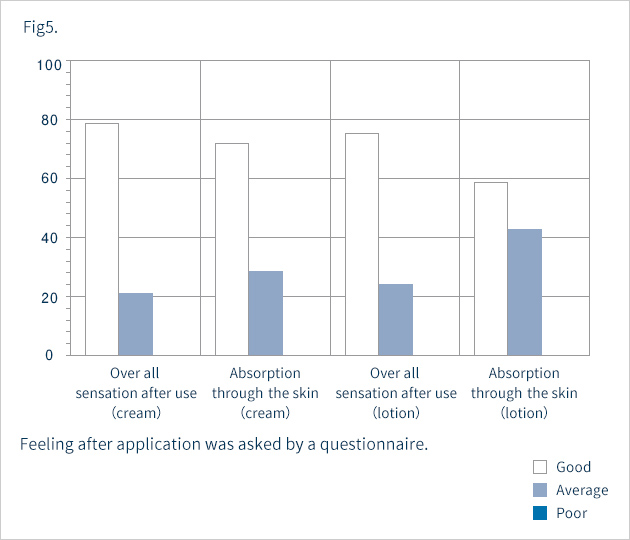
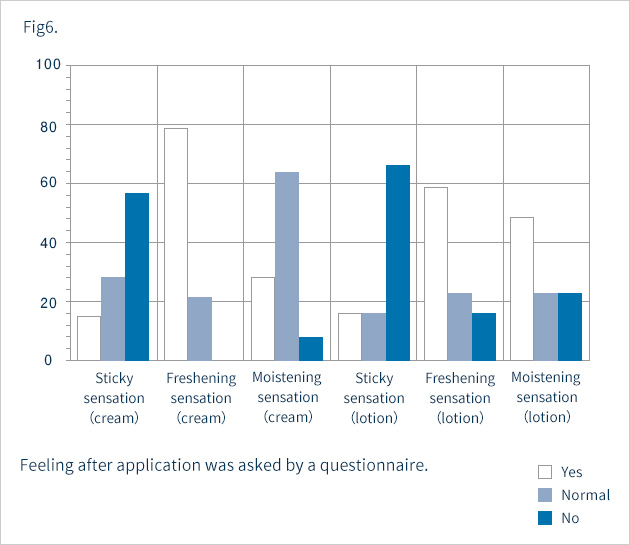
Assessments were made four weeks after the start of topical application. Erythema, scale, and itching were grouped into the following four categories: 0=none, 1=mild, 2=moderate, 3=severe. Overall improvement was classified into the following five grades: 1=markedly improved, 2=improved, 3=slightly improved, 4=unchanged, and 5=exacerbated. Safety was graded on a scale of 1 to 4: 1=safe, 2=nearly safe, 3=questionably safe, and 4=unsafe. On the basis of overall improvement and safety, usefulness was assessed as 1=highly useful, 2=useful, 3=slightly useful, 4=useless, or 5=unfavorable. At the end of the study, we issued a questionnaire on the patients' sensations after topical application. The questionnaire requested respondents to express overall sensations experienced after use and absorption through the skin as 1=good, 2=average, or 3=poor. Whether patients felt a sticky sensation, moistening sensation, or freshening sensation was also inquired about with the following responses possible: 1=yes, 2=neutral, or 3=no. Corneum water content was measured with a Skicon-200.
■Results
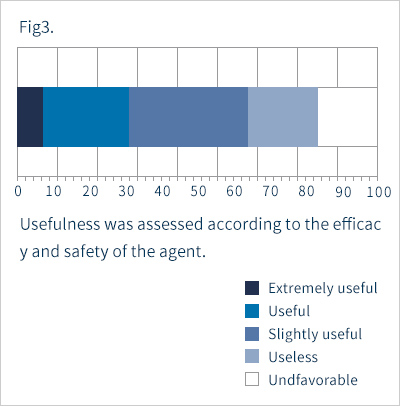
Fig. 1 shows the overall improvements. Seven percent, 20% and 40% of the subjects showed marked, moderate and slight improvements, respectively. That is, 67% of the subjects showed some improvement. The disease remained unchanged in 20%, and was exacerbated in 13%. Of the six patients with severe cases of the disease, only one patient showed improvement, four were listed as "unchanged" and one was "exacerbated" As shown in Fig. 2, itching and erythema improved significantly after topical application. The score for scale was improved, but not significantly. Two patients showed exacerbation presumably due to irritant contact dermatitis, while the other five had only mild skin irritation. Taking safety into account, the response rate for "slightly" or more useful was 67% (Fig. 3). In five patients, we measured the corneum water content, which was found to be slightly increased after application, but not to a significant level (Fig. 4). Figures 5 and 6 summarize the results of the questionnaire-based survey. With cream and lotion, the percentage of patients reporting a “good” overall sensation far exceeded those reporting an “average” one, and no patients answered “poor”. With respect to absorption through the skin, more patients answered that the cream was “good” than they did for the lotion, though none answered “poor”. Many of the respondents experienced no sticky sensation with either cream or lotion, though some reported “yes” when asked about a sticky sensation. For moistening and freshening sensations, more subjects answered “yes” or “neutral” for the cream than for the lotion, with some responding "no" for the latter.
■Discussion
Atopic dermatitis is usually treated in three ways. The first is the control of inflammatory manifestations by the external application of anti-inflammatory agents such as steroid hormones. The second treatment procedure is the removal of the causative agents. The third procedure is appropriate skin care, which includes protecting the skin from dryness and maintaining its barrier function in the healthy condition by keeping it clean and applying water-retaining preparations topically. Skin of the patients with atopic dermatitis is generally dry, mainly due to a decrease in the water content of the stratum corneum. In addition, transepidermal water loss (TEWL) is increased in this disease. These changes result from reduction in the amount of natural moisturizing factors, which are mostly amino acids, and of ceramides that occur in intercellular spaces of the corneum. The changes have been ascribed particularly to a decrease in the major constituents of sphingolipids, ceramides3-5), 8-12). The decrease presumab arises, not from the increase of ceramidase activity10), but from the reduction of ceramide-producing sphingomyelinase (SM ase)11) and the increase of sphingomyelin (SM) acylase. When the sphingomyelin acylase increases, the metabolism of sphingomyelin occurs in the non-ceramide sphingosyl-phosphry1choline production pathway resulting, a fall in the level of prosaposin12) . The decrease in ceramides is thus considered to be one of the important causative factors of the drying of the skin in atopic dermatitis. Therefore, the topical application of preparations containing ceramides on atopic dry skin should serve as an effective treatment. In the present study we used glycoceramide, which is capable of retaining water. Although glycoceramide does not naturally occur in the corneum, it is presumed to be converted to ceramide in the epidermis which retains water. The finding that topical preparations containing cermadide are effective against atopic dermatitis suggests that the compensation of ceramide loss woule useful for controlling the skin manifestations of atopic dermatitis. However, since the topical preparations left unchanged or exacerbated severe atopic dermatitis, they should be used only in moderate or mild cases of the disease.
References
- Horikawa T, Ichihashi M.: Environmental factors and atopic dermatitis. Environ Mutagen Res, 18: 91-95, 1996 (Japanese)
- Watanabe M, Tagami H, Horii I, Takahashi M, Kligman AM: Functional analyses of the superficial stratum corneum in atopic xerosis. Arch Dermatol, 137: 1689-1692, 1991
- Imokawa G, Abe A, Jin K, Higaki Y, Kawashima M, Hidano A: Decreased level of ceramides in the stratum corneum of atopic dermatitis: an etiologic factor in atopic dry skin? J Invest Dermatol, 96: 523-526, 1991
- Osawa J, Takahashi M, Ikezawa Y: Pathological approach atoatopic dermatitis from aspects of skin barr ier disturbance and dry skin. Treatment of Atopic Dermatitis (Ikezawa Y, ed.), Life Science Medica, To kyo, 1997, pp31 - 34(Japanese)
- Matsumoto M, Masamoto K, Umemoto N, Sugiura H, Uehara M: Epidermal and intercellular lipids of the stratum corneum of patients with atopic dermatitis: comparison between groups with or without complicating ichthyosis vulgaris. Bull Dermatol, 91: 155-158, 1996 (Japanese)
- Seguchi T, Cui CY, Kusuda S, Takahashi M, Aisu K, Tezuka T: Decreased expression of filaggrin in atopic skin. Arch Dermatol Res, 288: 442-446, 1997
- Tagami H, Iwatsuki K, Kanamaru Y, Yamada M, Ichijo B: Evaluation of the skin surface hydration in vivo by electrical measurement. J Invest Dermatol, 75: 500-507, 1980
- Imokawa G: Structure and function of intercellular lipids of the stratum corneum. Oil Chem, 44: 751-766, 1995 (Japanese)
- Yamamoto A, Serizawa S, Ito M, Sato Y: Stratum corneum lipid abnormalities in atopic dermatitis, Arch Dermatol Res, 283: 219-223, 1991
- Jin K, Higaki Y, Takagi Y, et al.: Analysis of beta-glucocerebrosidase and ceramidase activities in atopic and aged dry skin. Acta Derm Venereol, 74: 337-340, 1994
- Murata Y, Ogata J, Higaki Y et al.: Abnormal expression of sphingomyelin acylase in atopic dermatitis: an etiologic factor? J Invest Dermatol, 106: 1242-1249, 1996
- Chang YC, Kusuda S, Seguchi T, Takahashi M, Aisu K, Tezuka T: Decreased level of prosaposin in atopic skin. J Invest Dermatol, 109: 319-323, 1997